Category Archives: Entries
November 2013
Written by Weijia Chua (class of 2013-2014)
THE LECTURE
Dr. Harken’s Friday morning lecture began promptly at 7:15am. He spotted me, came over to introduce himself and warmly welcomed me for the day.
Dr. Harken opened the lecture with a question: which would heal faster, a cut in the toe of a diabetic or a cut in the scalp of one of our residents after we have spit into it? (Dr. Harken kept the lecture entertaining with his playful sense of humor) The residents all agreed, diabetes decreases blood flow, so injuries are slower to heal in diabetics than in people who do not have the disease. His follow up question, however, was trickier: is it the difference in blood flow or difference in exposure to oxygen that allows the resident’s wound to heal faster? If you could only increase blood flow without increasing oxygen exposure or only increase oxygen exposure without blood flow, which would you choose?
As I began to ponder in what real-life situations would a physician have to choose between one or the other, when the two seem so clearly linked, Dr. Harken started to make his point by presenting a retrospective case study: in 1993 a hospital encountered 300 patients who had gone into septic shock. Of the 300, 85 survived and 215 died. Aside from the ~75% mortality rate, what was striking about the data was that all the survivors were reported to have had a natural cardiac output of greater than 6L/min, while all those who did not, reported a natural cardiac output of less than 4L/min. “After seeing this data, are you convinced that you should treat septic patients by increasing their cardiac output? How would you design a study to test your hypothesis? Is it ethical to put patients in the control group (ie. no treatment/increase of cardiac output)?” he asked.
After some deliberation and teasing from Dr. Harken about the residents’ inability to come to a consensus—something surgeons will need to learn how to do as they make decisions about unclear cases as a team—Dr. Harken presented the follow-up study in which the control group was given standard treatment (no increase in cardiac output) with a resulting mortality rate, again, of 75% and the treatment group’s cardiac output was artificially increased with a resulting mortality rate of 40%, showing that stimulating cardiac output indeed improved the outcomes
of sepsis patients. I noticed that Dr. Harken did not explicitly provide “correct” answers to any of the questions he posed, which may have been his way of saying that medicine often does not provide us with black and white answers. However, I took his presentation of the follow- up study to mean that, in his opinion, it was okay to put patients in the control group in order to study and establish better treatment standards.Finally, Dr. Harken brought the lecture back to his original question by presenting two final studies. The first showed that artificially increasing oxygen delivery to normal physiological levels led to a mortality rate of only 15%, even lower than that from increasing cardiac output past normal levels. The second showed that artificially increasing oxygen delivery past normal physiological levels, however, did not improve patient outcomes as predicted by some physicians at the time.
While the day’s lecture seemed to be somewhat unrelated to surgery, I realized there were many universal lessons that Dr. Harken’s talk brought to life: 1) study design (and medicine in general) can be tricky and involves many variables, including ethical implications 2) you must be cautious of the conclusions you make from studies and know how to not over interpret data and 3) my personal favorite: more is not always better. These valuable lessons stayed with me as I observed the decisions that the physicians made throughout the day.
GETTING STARTED
After the lecture, a crowd of residents formed around Dr. Harken, each with questions or thoughts they wanted to discuss with him. Unsure of whether to wait or not, I decided to head up to the OR by myself.
Because I arrived alone, I rang the bell on the speaker, even though my badge was able to open all the doors. I introduced myself to Nurse Wendy and she buzzed me in, showed me the loaner scrub card and how to get scrubs out of the scrub vending machine right outside the women’s locker room. She explained that I would need the same card to return the scrubs at the end of the day, and to just ask for it at the front office. I got changed, threw on a pair of shoe covers and what looked like a non-waterproof shower cap (found next to the scrubs machine), and Wendy showed me to OR 5, at the order of Nurse Julie. Before entering the OR doors, I put on a mask with an attached eye guard (found above the sinks outside the ORs).
Wendy introduced me to the residents assigned to OR 5 for the day: Dr. Muriel Babey, a first year resident, and Dr. Jessica Williams, a second year resident. I also met Matt, a nurse who was the circulator also assigned to OR 5 for the day. Like Connie, I ended up sticking with the same team and OR 5 for the day and Matt really enhanced my experience by helping me to find a good position to watch from and providing explanations for what I was observing.
FIRST SURGERY
The patient, a 59 year old Filipina woman, was already lying sedated on the operating table when I entered the OR. She was very thin, petite, and had a delicate looking build that instantly reminded me of my grandmother. Dr. Williams showed me her chart and explained that this surgery would be a re-excision on a recent lumpectomy. She had been diagnosed with breast cancer and had a tumor removed (lumpectomy) about 2 months ago. A follow- up mammogram showed that the original surgery did not remove the outermost edges of the tumor, and thus today’s surgery was scheduled in order to remove what was missed last time. I was surprised to learn that the need for re-excision surgery is quite common, at a rate of about 50%. Dr. Williams explained that this type of surgery is considered an art since surgeons cannot visually identify tumors even when they open up a woman’s breast tissue. In this particular case, the surgeon would have to find the cancerous tissue by touch.
Dr. Sajadi was the attending presiding over the case, but he mostly observed and advised Dr. Williams as she performed the surgery. She began with a small horizontal slice above Ms. S’s right nipple and Dr. Sajadi held the cut open as Dr. Williams used a cauterizer to separate the tissue from the skin and to remove two 1inch by 1inch chunks. These tissue chunks’ orientations were labeled with sewn in threads by the surgeon and sent off to pathology. Although the patient has DCIS: Ductal carcinoma in situ, the earliest form of breast cancer, Dr. Williams explained that her case was not a straightforward one and a committee would have to take a look at the tissue pathology results and discuss whether a mastectomy would be needed as part of her future treatment.
But for the present, Dr. Williams cauterized back some tissue to help the closure sit evenly, sewed the patient up like an expert, and injected some type of clear fluid that seemed to inflate the hole that had been created by the tissue removal. The anesthesiologist then woke her up. In total the surgery lasted only thirty minutes!
SECOND SURGERY
After my first surgery, there was an unusual lull in the surgery schedule. Every single OR was empty as each of the scheduled surgeries was somehow delayed due to unexpected circumstances or complications. Curious, I headed to the patient area, where I met a young man in his late twenties waiting to receive a skin graft on his recently operated on legs. He shared that he made his living as a caregiver and hoped to be able to walk again soon so he could return to work. I could tell that his profession suited him well as he spoke warmly and pleasantly and displayed a great deal of patience despite his difficult situation. His surgery had been delayed several hours as he had had an allergic reaction to the pre-surgery antibiotics his surgeon had given him. His team was now trying to find him a suitable antibiotic by testing small amounts of different ones on him and waiting to see if he would react. The poor guy had already reacted to three by the time I saw him.
In the bed next to the patient, a patient whose surgery I would be observing next. She was a 52 year old African American woman who would be receiving a lumpectomy to remove a region of possibly cancerous calcifications from her left breast. She was clearly concerned about the surgery and expressed adamantly that she did not want to be intubated. Dr. Williams’
first response was to kindly ask, “Why?” It was then that we discovered that the patient’s passion was singing in her church choir and she was worried that a breathing tube could even slightly damage her vocal chords. Dr. Williams gently outlined the pros and risks of each of her anesthetic options with specific attention given to the effect it could have on her vocal chords. She then gave her some time alone to make her decision. From what I gathered, she had little to be concerned about. However, I was touched by how serious Dr. Williams took her patient’s concerns and could see how far not only the conversation, but also her demeanor went in easing her mood and preparing her mentally and emotionally for surgery.
This second surgery was similar to the first, yet differed in that the mass to be removed could not be identified by touch. Instead, X-ray was used to visualize the tissue and insert a metal hook into her breast tissue that would act as a marker for the region containing the calcifications. Dr. Babey and Dr. Sajadi were then able to use the X-ray (aka. Mammogram) pictures and the hook to guide their cutting. I felt silly thinking this, but I was truly amazed at the beauty and effectiveness of such a simple low tech method.
This time, the removed mass was sent to X-ray. And after thirty long minutes of waiting, we received the good news: X-ray showed that the mass removed indeed contained all the expected calcifications. Success!
THIRD SURGERY
The third surgery I observed was an emergency one that bumped down the next case that was originally scheduled for OR 5. It was officially termed a “decompression of the corpus cavernosa” by Dr. Das, the attending who would be performing the procedure. However, none of the other staff in our OR had ever seen or knew of the procedure.
The patient was a 22 year old male who had arrived at the hospital with an erection that would not go down. (It was unfortunately also his birthday that day.) He displayed very little emotion as he described the pain and sensitivity he was feeling. The doctors were unsure of what had caused this, as the only suspecting substances he had had the day before was alcohol
and marijuana—not known to be related to prolonged erections. Dr. Das mentioned that they sometimes see this happen in patients that have sickle cell anemia, as the sickled blood cells can cluster and block the vessels leading out of the penis causing blood to collect there. However, he did not have sickled cells and none of the men in his family had ever experienced this before.
While the cause was a mystery, what needed to be done was not. The corpus cavernosum is one of a pair of sponge-like regions of erectile tissue which allows the penis to become erect when filled with blood. If the penis remains erect for too long, it means that blood has pooled there and is not circulating through the tissues. Without blood circulation, the tissues will eventually die.
Thus, the plan was to surgically drain the blood from his corpus cavernosa, though there was a possibility that he could still lose the ability to have an erection in the future.
Dr. Das began the procedure by inserting a needle into each side of the penis and squeezing it to force the blood out through the needles. Every five minutes he injected a small volume of phenylephrine, which was meant to constrict the blood vessels entering into the penis in order to hopefully stop blood from continuing to enter into the corpus cavernosa. Once blood was no longer flowing out from the needles, Dr. Das made a series of incisions along the length of the penis and suctioned out the blood. Once the penis was finally drained, he sewed up the incisions and then bandaged up the area, thoughtfully leaving some leeway room in the bandage for when Mr. N would have to urinate.
I unfortunately had to leave at this point, and did not get a chance to see the patient wake up from the surgery.
TIPS?
-Just wanted to second what Connie mentioned about the circulators, moving around the OR, and sticking with the same team/OR for the day.
-Residents Dr. Williams and Dr. Babey mentioned to me that the breast cancer cases are usually scheduled for Fridays and they even offered to let me shadow them in the breast clinic that afternoon. If you are interested in breast cancer, then maybe Fridays would be a good day for you to come in.
-I thought the OR board would have the start time for each surgery, but I realized that there weren’t any times listed because I am guessing that it can be difficult for the staff to predict how long surgeries will take and sometimes preparation complications arise, delaying the start of surgeries. I figured out that they erase the surgeries off the board once they’re finished, so whatever surgery is listed first under an OR is either currently going on or about to happen. I would say, if you see a surgery you are interested in, peak into the window of its OR. If it hasn’t started yet, head into the patient area and look for the patient. You’ll be able to find them because there’s a brightly colored card with their OR# displayed next to their bed. You can chat with them and observe the doctors prepping them for surgery. Then you can just follow the patient from the prep room into the OR so you’ll be sure to not miss a thing.
February 5, 2013
Written by Jon Zaid (class of 2012-2013)
When I first arrived to the conference room the residents and the students were engaged in a conversation led by Dr. Palmer regarding different approaches to post-op antibiotic treatment and how the goal is to pick the right dose with an aggressive regiment. However, there are also damaging repercussions if the antibiotic therapy is either too potent or too long in duration. This made me think about how surgery is a very technical skill but that is not all there is to being a surgeon. Interviewing patients and getting to know them prior to surgery allows the doctors to determine how compliant may be with post-op therapy or the antibiotic regiment. Highland is unique in that the types of patients that are seen tend to be poorer and less educated, and with that is a correlation to be non-compliant with prescribed courses of action. This presents an interesting hurdle for doctors in these types of areas, as opposed to doctors and surgeons in more affluent areas in which patients can recall their medical and family medical histories with greater accuracy, and are also more likely to follow up in the proper manner. Speaking with Dr. Palmer afterwards, he told me that no two surgeries are ever exactly the same, not only because the patient’s anatomy is different, but their medical and social history is different which can sometimes add complicating factors during and after surgery.
The first surgery of the day was a right portal catheter placement by Dr. Stam. The patient was a 55 year-old female who was recently diagnosed with breast cancer, and the catheter was to be placed to make infusion therapy more tolerable. Working in an ER, I am able to see many patients that come in with the ports already embedded in the chest and I’ve never had the opportunity to see how the ports get there in the first place. I should first describe the reason for ports to be inserted in the first place. Cancer patients undergoing chemotherapy will have infusion therapy sessions each week in which they are stuck with an IV that continuously delivers the chemical cocktail into their veins over the duration of the session. When getting “stuck” in the same veins over the course of chemo treatment, veins can get hardened from the repeated traumatic poking and can become more and more difficult to be a viable route for chemo. A port cath is literally a plastic ring that is directly linked to a major vein that gets inserted beneath the skin. Now a nurse can initiate infusion therapy through the port to deliver the cocktail to the patient, rather than having to find veins in the arm. In this case the jugular vein is connected to the catheter so that the drugs can be most effectively distributed to the body once it reaches the heart and is distributed systemically after reaching the left ventricle. When the course of treatment has ended and the patient is cancer-free, the port is removed.
The procedure itself was interesting, as it was the only one that the staff (including myself) had to wear lead vests throughout the duration so that X-rays could be taken frequently to verify that the catheter is correctly positioned into the jugular vein (JV). First a small incision is made below the right clavicle and a wire is fed into the JV with the aid of ultrasound. Then a 2cm incision is made about 6cm below the initial incision where the port is inserted. Then beneath the skin a path is created between the first incision and the port where a catheter tube connected to the port is pushed through to where the first incision and the wire is situated. X-rays are used to verify that the wire is indeed going into the JV at this point. Then the wire is removed but replaced with a larger hollow tube using a gun-like device. The catheter connected to the port is then fed into the larger hollow tube, which is in the JV. The upper chest is then X-rayed again to verify the placement of the port cath as well as ensure that it does indeed connect to the JV. The port is then sutured to the subcutaneous layer and then is flushed with a heparin solution. The heparin solution is an anti-coagulant, which is used to make sure any blood that makes it into the catheter does not clog the newly placed cath. Once that is complete the skin over the port is stitched up and the entire procedure only took about 45 minutes. The patient’s life is now made easier after a simple outpatient operation that was facilitated by amazing technology that wasn’t around 20 years ago.
The next procedure was a wide local excisional biopsy of a large “melon-sized” liposarcoma on a 39 year-old male by Dr. Bullard and Dr. Rahbari. The tumor was so large that many other staff-members came in to see it, and even Dr. Palmer took several pictures of it from different angles because of its unusual size. Although the surgery seemed pretty straight forward, it was interesting because once the first incision was made (about 2cm surrounding the black necrotic skin), the only way to tell how deep into the leg the tumor penetrates is by feeling for hardened material below the surface. Therefore it is not straightforward and some difficult decisions needed to be made regarding how deep into the leg should be excised. Dr. Bullard and Dr. Rahbari had to be in constant communication because the tumor was so large that each cut needed the support of the other doctor to hold the weight of the tumor to ensure that no vital arteries are accidentally sliced. During the excision, I could see various leg muscles twitching, which I had never seen before. Almost the entirety of the anterior skin of the left thigh was removed so it looked as if I was in an anatomy lab. The doctors were pointing out various aspects of leg anatomy to myself and the students as it is not often that we are able to get the opportunity to view such a large portion of an exposed area on a living person. After the 3 hour surgery was complete a mass about 15x 25×13 (or the size of a football) was removed from the patient and placed in a bucket. The estimated weight was about 8lbs. To identify the proper orientation of the removed mass on the body once it was removed, the medical student made long stitches on the lateral aspect and short stitches on the superior aspect. The large exposed area of the thigh was then closed like a corset with some of the exposed muscles simply covered with damp dressing. The patient had much of one his thigh muscles completely removed, but would be able to walk again with physical therapy and he would now hopefully be cancer-free. Another aspect of serving in poorer areas is that patients can often come to see a physician well after they should have initially sought medical evaluation. This makes for more acute illness and perhaps more interesting (from a medical standpoint) cases such as the large liposarcoma. This goes back to what Dr. Palmer had told me earlier in the day about no two patients or surgeries being exactly alike. I was able to see two very different cancer patient’s lives hopefully improve a lot today in two very different ways.
March 2013
Written by Sonia Spindt (class of 2012-2013)
I thought I could forget about physics after I took the final for that class last spring. Most of the topics covered in my class seemed to be surrounded by facts that I, nor any other pre-med student, would ever use again after taking the MCAT—there was always a question of relevance present when studying physics’ material. However, Dr. Harken surprised me when he began his morning lecture with the question, “what is Ohm’s law?” Sadly, my mind drew a blank! Thankfully, the residents remembered that the equation simply states R=V/I. My mind quickly reverted back to last spring and I immediately began to struggle with an issue of relevance here. How could a patient’s health fit into this equation that talks about the behavior of circuits? According to Dr. Harken, Ohm’s law can be modified to discuss Systemic Vascular Resistance (SVR) and its roll in shock. In this case, the resistance found in the systemic vasculature of a patient would be equal to (Mean Arterial Blood Pressure (MABP)-Central Venous Pressure(CVP))*80/Cardiac Output (CO). All of these can be measured to determine if the patient falls into the normal SVR range of 800-1200 dyn. Having set the stage, Dr. Harken then went on to describe the following three scenarios:
Patient 1
A patient comes into the emergency department with a BP of 90/60, a MABP of 74, a CO of 4 L/min., and a CVP of 4. What is his SVR? What is the subsequent plan of treatment? After using the above equation, the physician would find that the patient’s SVR is 1400 dyn, a value that falls above of the normal range. In this case, the increased SVR is indicative of hypovolemic shock, or having a state of decreased blood volume. Consequently, the treatment would simply be to give the patient more volume. The causes of hypovolemia can include: external/internal bleeding, severe burns (leads to a loss of plasma), loss of body sodium and intravascular water (vomiting, diarrhea, sweating), and vasodilation (can happen after a trauma inhibits the vasomotor center in the brain).
Patient 2
A patient comes into the emergency department with a BP of 85/60, a MABP of 62, a CO of 4 L/min, and a CVP of 12. In this case, CVP falls into a normal range, so no additional volume is needed. The physician notes this difference and calculates the SVR for this patient and finds that it is 1,000 dyn. Some additional tests would have to be performed to confirm that this patient is experiencing cardiogenic shock, a type of shock that implies that there is inadequate circulation of the blood. In this case, the patient’s doctor would order a Beta 1 agonist to increase the heart’s pump action.
Patient 3
A patient comes into the emergency department with a BP of 85/60, a MABP of 62, a CO of 8 L/min, and a CVP of 12. The doctor calculates the SVR to be 500 and notices that the patient is warm. The doctor concludes that the patient has an infection and is experiencing septic shock. In this case, the doctor would order an Alpha agonist.
Essentially, Dr. Harken used these scenarios to argue that three types of treatment should be considered when a patient exhibits symptoms of shock. Ultimately, the doctor should 1. give the patient volume, 2. administer a chemical agent like a Beta 1 or Alpha agonist, or 3. increase hemoglobin to increase oxygen saturation. In the medical field, this is called “Early Goal Directed Therapy” and Dr. Harken is a firm believer in this system of treatment. It was nice to hear this lecture because it reminded me that even the smallest of things learned in our undergraduate years can still be important in a later career. The morning meeting was soon finished and I made my way up to the OR.
While looking at the board, I ran into Dr. Krosin, who immediately told me that I should go to OR 3 to watch a Tram Flap Reconstruction. I eagerly took his advice and dashed off to OR 3, where the very jolly Dr. Allen greeted me. I explained who I was, and Dr. Allen happily volunteered to describe the procedure and to answer any questions that may arise during the 6 hour surgery. Of course, I was curious about the patient’s history, so I asked Dr. Allen about her story. The patient was a 38 year old woman who had had a mastectomy because of breast cancer. She opted for reconstruction with an expander (an implant) but that soon failed when the implant became infected. Dr. Allen offered to try the expander again but sadly, it too failed. The state of the breast tissue was too mangled by infection to be salvaged, so Dr. Allen suggested the Tram Flap Reconstruction. The patient was very hesitant at first to undergo this extensive procedure, and after watching the surgery, I don’t blame her.
Dr. Allen first began by removing the infected expander from the patient’s left breast. He removed the infected issue and scraped/irrigated the resulting cavity. After this, he began to cut out a section of the patient’s abdomen, to mobilize the rectus muscle. There is a crude drawing at the end of my journal to help illustrate the size of the piece of abdomen being removed (about 25 cm by 25 cm). It was divided up into four quadrants, two of which would be utilized for the breast reconstruction. For the next 2 hours, Dr. Allen and his resident began to slowly expose the abdominal wall found beneath the mesentery and fascia. A few times during the procedure, Dr. Allen would excitedly point out the amazing anatomical features found in this surgery, asking me to literally stand next to him, only inches away from the table. My favorite point in the procedure was when Dr. Allen was clipping blood vessels that were entangled with nerves. Every time Dr. Allen cauterized the vessel with the bovie, the electricity found in the tool would cause the rectus muscle to violently contract. It was really exciting to see this because it was only something I hypothetically read about in my physiology textbooks. Here I was, standing an inch away from a human muscle that was very alive and very active. When the piece of mesentery was finally free from the patient’s abdominal wall, Dr. Allen asked me to stand by his side again so that he could point out the infamous linea semicircularis. According to Dr. Allen, this is one of very few surgeries where this line is exposed.
After this, Dr. Allen had to make a tunnel from the abdominal flap up to breast cavity. It essentially had to be a hole big enough for a human fist to fit through and it had to transverse the entire human torso. To do this, Dr. Allen took both of his fists and pushed them into the patient until they were touching. As you can imagine, Dr. Allen had to vigorously shimmy his arms through the patient’s torso and of course, he worked up quite the sweat doing this. Once the tunnel was large enough, he lifted up the abdominal flap and rotated it 90 degrees, so that the rectus muscle was essentially lying 180 degrees on top of itself. From here, he started to push this baby-sized piece of tissue through the tunnel until it emerged from the breast cavity. At this point, the anesthesiologist, all of the nurses, the graft specialist, Dr Krosin, and I were all silently watching this amazing feat being performed. It was an ingenious technique that allowed for the healthy vascularization of the new breast tissue and stability of said tissue from the rectus muscle found beneath. It allowed the breast to feel natural and it had the added bonus of a tummy tuck. Of course, this procedure was insanely invasive, and the pain would be about the same as the pain felt by those who are struck by trucks.
For the next two hours, the surgical team worked on closing the patient. A graft made from pigs skin (which was the same price as a Ford Focus) was needed to help close the abdomen. Dr. Allen essentially removed quadrant 3 and 4 from the abdominal flap, now found in the breast cavity, because they were edge pieces and not as well vascularized as the inner 1 and 2 quadrants. This surgery was by far the most exciting surgery I have seen, and I highly recommend watching Dr. Allen perform a Tram Flap Reconstruction if given the chance.
January 2013
Written by Seungwhan Alex Roh (Class of 2012-2013)
The first OREX shift of 2013 started out as usual with me arriving early to the conference room and introducing myself to Dr. Harken. Dr. Harken, as usual, was lively as ever and seemed to be full of energy so early in the morning. Just like the last two times, the residents all poured in at once as soon as the clock struck 7:15am. The topic for today was hyperglycemia in regards to septic shock. Dr. Harken started out by briefly laying out the normal conditions of the body. He described how during clean stress, the body increases blood glucose level by emptying out the glucagon storage in the liver and converting it via gluconeogenesis. Then he laid out four different situations of stress: starvation, clean injury, a high intake of calories with high metabolism, and septic injury. According to reports, only septic injury seems to cause a different stress response than the previous three and it is what most surgeons encounter during their operation. After some discussion, he moved onto his next point which was whether hyperglycemic conditions were better for septic injuries. He shared various journals that had done studies upon the topic and saw that overall, people with chronic hyperglycemia did not fight against infections as well as normal patients. He then went unto further discussion on what we could do to get conclusive evidence. Finally, he ended the discussion by stating what the current status was, that during septic shock hyperglycemia is either a control mechanism to counter the shock or a result of endocrine homeostasis failure.
As the morning discussion ended, I quickly went up and changed into scrubs to see what the available surgeries were for the day. There were two that caught my eye immediately, but I ultimately went towards the ACL repair since, as a sports fanatic, I have frequently heard of athletes getting ACL repair. The official full name for the operation was right arthroscopic anterior cruciate ligament repair with meniscal repair and debridement. The patient was already put into unconsciousness when I arrived and the medical staff was getting ready for the operation. The setup for the operation took longer than usual since the tourniquet had to be put onto the right leg and also the foot had to be wrapped tight to have the rest of the blood from being pooled there. They covered the entire patient with the sterile blue sheets as usual and only left he knee joint exposed. At the start of the operation, I did not see Dr. Krosin, who was supposed to be the attending physician for the operation, but only Dr. Wang, the senior resident. He began by marking the incision spot (inferior and medial to the patella) and making the incision with the scalpel. Then he started harvesting two tendons, the gracilis and the semi tendonitis. He carefully scraped along the tendons, making sure no damage to the actual tendon occurred. As soon as the attachment points for the tendons near the incision was freed up, Dr. Wang sutured up the end of the tendons individually. Then he proceeded to pull the tendons while scrapping up the other attachment point with a metal rod with a loop to complete the harvesting. At that point, Dr. Shah entered to help Dr. Wang with the rest of the surgery. The two tendons were then allowed to soak in saline to prevent it from drying out. A few minutes later, two other physicians, one attending (I believe Dr. Krosin?) and one resident, entered the room. The team then decided to switch directions and decided to do the ACL repair with an autograft (using the nerve from the patient’s body) rather than the allograft (using a nerve from a donor). The only problem with the decision was that the box that contained the allograft was already opened so the team wasn’t sure if that allograft was returnable or not.
With that confirmed, the team split into two. Dr. Wang proceeded with the meniscal repair and debridement while Dr. Shah prepared one of the two tendons as an autograft. For the meniscal repair, Dr. Wang inserted a camera in the joint and used a rotating suction and a grappler to clear away the damaged tissue. The whole area was flooded for the camera and the suction. Interestingly, the images displayed on the screen looked similar to the images for an underwater flora as the damaged tissue waved back and forth like an anemone that was moving with the ocean current. The images displayed were also very crisp as the cameras were capable of high definition and registered no lag. The downside of the camera was that it had to be moved around manually and so it was hard to control. This meant that there were moments when it took time to position the camera so that the operation could be seen clearly. This also resulted in a longer period of debridement as the camera had to be moved around quite frequently to survey which tissues had to be removed.
While Dr. Wang went on with his work, Dr. Shah began preparing the autograft. He first scraped off any extra tissue stuck onto the nerve with the edge of a scissors and rinsed the nerve with the saline. Then, with the instruction of the other attending physician, he began making suture crosses at the end of the nerves. This was so that the team could have a firm grasp of the nerve. The nerve was tested at the end by applying tension to it and seeing if it could handle the tension.
As soon as both of the tasks were finished, Dr. Wang grabbed a drill and drilled a hole through the head of the fibula. Once inside the joint, the drill folded into a 90° angle and Dr. Wang partially drilled back to create an even bigger opening that spanned halfway. This was where one end of the nerve was going to go. This end was going to be held up with a pin that would clamp itself in the opening and would allow the nerve to stay. The other end was going to be attached with a screw and would determine how much tension the nerve was going to have. The screw itself was white and made with the latest technology, made with a biodegradable material that would be completely absorbed by the body in two years. When the graft was inserted, the pin stuck right away in the correct position. It was interesting to see with how much force both Dr. Wang and Dr. Shah pulled on the sutures to test the strength of the pin and the nerve. It really showed how strong the human body was. Next, Dr. Wang drilled a hole through the tibia so that the screw could be put in place. Once the nerve was set in place, the team took several photos of the result and the operation was deemed successful. The incisions were sutured up and a caste was put on the leg. Overall the entire operation took a little less than 4 hours to complete.
As the team was finishing off, the physician was writing up the total bill for the operation. It was shocking to see how much each equipment cost and made me realize why most people wanted to avoid surgeries. If not for insurance, I could see why most people could not receive surgeries even if they wanted to. To see that one screw alone cost upwards of $300 seemed a little preposterous to me.
The best thing about the shift, however, was not the surgery itself but rather the conversations I shared with the doctors (and even just the conversation between the doctors themselves). It was cool to see what kind of activities that doctors enjoyed (and even better to know that it was the same activities that anybody else enjoys). Just the vibe that doctors were not always the serious and grave but also were cheerful and fun for some reason surprised me. Throughout the whole operation, the various doctors including the anesthesiologists came up to me and gave me various tips on the med school process and on which area of medicine I should choose. Overall, no day of OREX disappoints.
FEBRUARY 2013
Written by Manika Talati (2012-2013 Class)
There are some days you look back on and just know you will remember forever. You know the people, emotions, and environments you encountered will never escape your mind. My third OREX experience was exactly this type of day. Here is a recount of my experience.
It was 10:45 AM. I was scrubbed-in and all-ready for my first surgery observation. I went to the surgery board schedule, where I encountered Dr. Krosin, who I knew very well. He immediately exclaimed, “Manika Talati! How are you today? Check out the surgery on the trauma patient that just came in! You’ll probably see some brain.” He also recommended I watch the foot reconstruction he was performing that afternoon. I was so glad I ran into him! His advice gave me a direction to jump-start my day.
I proceeded to the trauma patient’s room. The environment was intense. The neurosurgeon and general surgeon were debating on performing a craniotomy versus craniectomy, technicians were diligently preparing the patient for surgery, and PA students were quietly standing to the side. I could tell this was a serious operation. The patient was a construction employee who suffered an extremely unfortunate injury that morning. A sledgehammer fell on him at work, creating a 4-inch wide opening exactly on top of his head. About a half-cup of internal tissue had escaped from the opening, which appeared bloody, chunky, and soft in texture. His cranium was also fractured from the impact. At this point I was curious to find out what the escaped tissue was. Blood vessels? Blood clots? Brain? I had no idea. The PA told me that it was in fact, his brain. She also explained to me that it was better the impact caused the skull fracture and escape of internal tissue. Apparently, if the cranium were completely intact, the internal pressure would be so high that there would be greater complications. Finally, the neurosurgeon decided to perform a craniectomy, or remove of part of the skull bones to access the brain. I have learned before that the human brain is very well protected. It was not until this experience, however, that this idea became clear to me. The skin on the head was strong and sturdy, about a half-inch in thickness. It was the opposite of the thin, easily pinch-able skin on our hands and feet. Underneath was the cranium. I could see the four distinct parts it had broken into that were completely detached from each other. I wondered, how are they going to fix this? What they did took me by surprise. The surgeons simply removed the bone pieces and continued incising deeper into the patient’s head. Apparently, in situations like this, it is more important to optimize the functions of what can be repaired, which involves sacrificing other structures. I now could see a translucent material, the dura mater, which was encapsulating soft brain tissue. Wow, I thought, I am actually looking at the brain! Yes, in front of my eyes was the structure that runs the human mind – every emotion, every thought, every part of human intelligence. It was so real, so alive, and so intact! As I looked closer, I noticed it was moving at a constant lub-dub pace, similar to a heartbeat. This was surreal to me. I appreciated the intricacy, potential, and vibrancy of the human body more than ever before at that moment. It is very rare one gets to experience situations like this, and I was utmost honored to be there.
Ultimately, the goal of the operation was rather simple. The first was to mesh escaped brain tissue into place. The second was to block internal bleeding. This involved using a “Doppler” machine to identify damaged blood vessels. After locating the veins, the neurosurgeon viewed them through a microscope to more precisely suture them. Next, he performed a ventriculostomy by inserting a catheter through the head to drain excess fluid. Lastly, he sutured the skin with strong stitching fibers. This marked the end of the operation. I did not even realize four hours had passed! I had been so captivated by the procedure! I felt like I could have kept learning, absorbing, and taking in everything from my surroundings. I felt so stimulated by all that was around me!
I knew exactly where to go next. I darted to Dr. Krosin’s surgery. I was welcomed with a lighthearted, casual atmosphere I knew to expect. With an iPod playing rock n’ roll, residents talking about “The Bachelor”, and Dr. Krosin’s friendly “Hey Manika! How’s it going?” greeting, I knew this was going to be quite different from the previous surgery. Dr. Krosin was performing a flat foot reconstruction to create an arch in the patient’s foot. The surgery was a lot more intricate than I expected! It involved manipulating tendons in the ankle to bend the toes, physically shifting the heel bone to the side to realign the foot, and drilling through the navicular bone to form a curved shape. It was like watching an artist who was dedicating immense knowledge, skill, and mental focus to create a masterpiece. At the end of the three-hour procedure, I noticed a clear difference in the patient’s foot, which now had the signature arch-shape. This observation experience, although not a life-threatening procedure, was as memorable and special to me as the previous. It was uplifting to see a noticeable improvement in the patient’s condition. Even more, Dr. Krosin showed me anatomical structures and answered my questions throughout the procedure. The surgery team even included me in their “Can you guess what song is playing?” trivia, which made me feel more comfortable. The environment was a mix of productivity, good-natured talk, and hard work. I felt a part of the medical team and also learned a great deal!
It was now 5:30 pm. My day was so stimulating that I was tempted to stay longer! Yet, I did have plans for that Friday evening. I decided to call it a day.
In retrospect, it is interesting to compare my two surgery experiences. While they seemed starkly different from each other, they were actually quite similar. Of course, the type of operation, medical specialties involved, and operating room atmosphere were complete opposites. The informal conversations and music jamming in Dr. Krosin’s room set a far more casual tone than the neurosurgeon’s. The surgeons’ contrasting styles reminded me of how people study in college. One student might prefer the academic library setting while another enjoys a casual coffee shop. The study style doesn’t really matter as long as they can both put forth their best effort. The same applies to surgery. Each may have their own style, and what matters is that they ultimately help the patient to the best of their abilities. This idea is well-captured by something each surgeon happened to mention that day. I remember the neurosurgeon saying, “At any moment, this man’s life can turn around”. Very true, I thought. He was literally dealing with life and death. Dr. Krosin, on the contrary, told me that as an orthopedic surgeon, he admits he is not necessarily saving lives. What he loves, however, is being able to “improve lives”. Both statements were simply stated, yet so true. They illustrate how all medical specialties are important in helping the human condition. I was honored to experience the two worlds in the same day!
April 2013
Written by Sonia Spindt (Class of 2012-2013)
As we all know, morning meetings with Dr. Harken can be somewhat hard to follow. He often lectures on topics that are both filled to the brim with acronyms and outside of our range of medical education. We frantically write down every word that is so easily uttered by Dr. Harken in hopes of being able to later put the pieces together when we attempt to write our journal entries. However, this morning meeting was not filled with the usual fragmented moments of comprehension. Instead, the topic was one that we all are familiar with as volunteers in a safety net hospital, health care for low SES populations.
My morning began when a lonely fourth year medical student, Allen, greeted me as I walked into the conference room. Not wanting to sit there in silence, I asked what was on the agenda for the meeting. Allen informed me that he was going to give a small talk on a project he started with some friends while in his first year of medical school. Being very intrigued, I asked about the project’s details and I eventually found out that the project was centered on ideas of media, social justice, and health care awareness. He and his friends videotaped individuals who lacked health care and were forced into unimaginable circumstances because of their low socioeconomic status (don’t worry, my mind also automatically jumped to Michael Moore’s documentary “Sicko”). Excited to actually be able to have a conversation that included more than just a “uh huh…?” mumble, I complimented Allen’s work and suggested that it could help tackle the issues created by the low national average reading level and the standards for health care literacy. Being somewhat impressed by my comment, he kindly invited me to participate in a survey on personal perceptions of health care that he would conduct after showing the room full of residents a clip. Dr. Harken briskly walked into the now full conference room, gave a short introduction, and let the medical student take the stage.
He began his talk with a two-minute clip of footage that contained the all too familiar stories of hard decisions brought on by a flawed health care system. For example, one woman was forced to choose what tooth to save because she didn’t have enough money to cover multiple procedures. (If you are interested in watching the clip or reading about the project please visit http://www.thevacuum.org/). After the clip, we all answered his survey that contained questions like “I agree with the idea of universal health” or “I am willing to pay more if it means everyone can be insured.” However, Allen was not prepared for the onslaught of critiques he would then receive from the residents who questioned the purpose behind such a study. Allen argumentatively stated that the project was used to try and influence public policy officials, a very lofty goal that often does not sit well with doctors who have been active in the field for a very long time and have witnessed very little change. Also, the residents were not moved by the footage that was deeply rooted in the rhetorical device of ethos. This reaction was not at all surprising to me considering the fact that every patient who walks into Highland has a story pulled from the same vein of bad luck. The doctors hear things like this on a daily basis, so the video was far from impactful.
Dr. Harken had prepared a lecture on the effects of giving patients fresh blood but was never able to make the transition into this topic because he was so enthralled by the public policy debate brought on by Allen’s research. Instead of flipping through the pages of a New England Journal of Medicine entry, Dr. Harken talked about the discontinuities found between the different sectors of the health care system. According to him, there are even discrepancies found between groups of doctors, (for example, those in the private sector versus those in the public sector), and that alone makes decisions hard because no one can every agree. I was amazed by the brevity of knowledge and the eloquence Dr. Harken possessed when discussing a topic like this on the fly. Soon the meeting was over and Dr. Harken could only tell Allen that he should figure out what his audience is and maybe add a question to the survey that asks when the surveyed individual last needed health care. I felt bad for Allen but it was definitely a nice change of pace for the morning meeting.
After grabbing some breakfast, I made my way up to the OR to watch my only surgery for the day, a simple lumpectomy. I targeted OR 5 because the surgeon and resident were just stepping out to start the process of scrubbing in. I don’t enjoy walking in on a surgery that has already started because I like to have a chance to introduce myself without feeling like I’m interrupting something. And this is important considering that befriending the surgeon can provide one with some amazing opportunities. Luckily this was just the case because as soon as I introduced myself, Dr. Godfrey invited me to scrub in with him…WHAT!?
Scrubbing in is quite the meticulous process, especially if it is your first scrub of the day. Being that this was my first scrub-in ever, Dr. Godfrey told me to take my time and count to 10 for each finger. Essentially, the entire process should take a little less then 10 minutes. To pass the time, he inquired about my background and where I was in the application process. He told me about his time in the Peace Corps and discouraged me from applying because the government doesn’t make the process all too enjoyable. We then talked about how he volunteers at a rose garden and we discussed the current events surrounding the Boston Marathon explosions, all of which just highlights the fact that Dr. Godfrey is a caring and very relaxed individual.
I clumsily made my way into the OR, making sure that my newly cleaned hands and arms remained isolated. The nurses giggled as I awkwardly attempted the proper suit-up procedure. There are ways to hold the towel as one dries each arm, applying a tricky flip maneuver to make sure one does not use the already contaminated side when drying the other arm. Surgical gloves come in specific sizes and I was said to be a size 7. One does not realize how difficult it is to put one’s fingers correctly into a glove when one is not given the chance to use the other hand! The nurses continued to giggle as they helped me sort out my fingers and finally, they tied my gown and told me to never lower my hands past my waist. And with that, my nose became suddenly very itchy and the surgery started.
Within seconds the resident started removing lymph nodes that were marked with a blue dye from the patient’s right auxiliary lymph nodes (the lymph nodes that are found right under one’s armpit. Dr. Godfrey asked me to come join him on the other side of the table so that I might better “see” the operation at hand. He took this as an opportunity to start “pimping” me, a term that is used to refer to the onslaught of questions asked by the attendee to the resident in an attempt to 1. teach and 2. restrain a large ego because we all know that medicine does incorporate some shame-based learning. Thankfully, he only asked me how many stages of breast cancer there are and being that my family is completely riddled with it, I easily told him, “four.” He smiled and started talking to me about the classification system used to describe each of the four levels of breast cancer. I swear that he used the term “Z11” when referring to the name of the national ranking system but after further research I can no longer definitively say this. Instead, it seems that I may have incorrectly heard “TMN.” Essentially, the patient was already classified as a level 2 because the mass in her right breast was already larger than 2 centimeters. This preliminary diagnosis would most likely be bumped up to a level 3 or 4 after the pathology confirmed that all of the lymph nodes harvested were positive for cancer cells. Dr. Godfrey took a break and let the resident tell me about closing a wound.
Due to the fact that they left a considerable amount of free space under the patient’s arm, the resident had to use 3 different types of stiches. The first was a deep tissue stich that essentially brought together the inner tissue of the lymph node, ensuring that no fluid would be able to build up in the wound. She only had to make 3 of these stiches before moving on to a dermal stich. Finally, she ended with a subcutaneous stitch. Dr. Godfrey then started on the lumpectomy and stressed using a blade because burning through the skin only prevents proper vascularization of the wound’s edges once it is sewn back together. When the surgeons got down to the tumor, they found that the cancer went much deeper than expected and this caused Dr. Godfrey to tell the resident that he wanted to really be a part of her recovery because the hospital was now at risk for litigation. Apparently, a test 2 years ago missed the cancer, allowing it to grow to a deadly size. Now she will most likely have to go through radiation, chemotherapy, and a complete mastectomy only to prolong her life and that was quite devastating to hear considering the fact that she was only 59. This cancer was completely avoidable if that original test was performed more carefully. They removed as much of the tumor as they could but they said they couldn’t clear the margins without performing a full mastectomy. Dr. Godfrey told the resident to only perform the dermal and subcutaneous stitch because they wanted the wound to fill with fluid. That way the breast would not have an awkward divot in it and the fluid would allow the breast to feel more natural. They then closed the wound and went to take a break. I thanked the team for their help and told them that it was an amazing experience to scrub in. I hope you all get the chance to suit up and I can not wait until my next day up in the OR.
June 2012 (Part 2)
Jimmy Lam, OREXer ’11-12
One of the symptoms of an OREX intern, I feel, is that you have a mild sense of insomnia the night before your observation. I guess it is because of the excitement and anticipation. I was actually up before my alarm went off at 6:30am. I got dressed and was out the door. I arrived at the 0A2 just in time. By 7:30AM the doctors and medical students begin to trickle in as they do. I was excited to see that Dr. Harken was lecturing today and I should be because the topic was about recovery and survival rates of patients with varying oxygen content in their blood. Dr. Harken started the lecture with the question, “what would heal faster, an incision on the head or the toe of a diabetic?” If you didn’t know anything about diabetics, you should know that a common and morbid effect of diabetics is the need to amputate limbs due to poor vascular circulation. Dr. Harken explained that the oxygen content in the blood makes a huge difference in the survival of the body or the organ it supplies. Dr. Harken then went in to describe a retrospective research that collected 75 patients that have been involved in an accident that caused the patient to drop to a blood pressure less than 90. The study then split the group into two, 35 patients were treated with standard levels of oxygen in their blood and the other 40 patients were treated with some chemical or hormone that increased their oxygen content to a hyper oxygenated state. The results of the studied showed that if you had your oxygen content increased either naturally or artificially, you had a 0% mortality rate in the operating room. Regardless if you were in either groups, if your oxygen content could not increase to the hyper oxygenated state, then you had a 30% chance of mortality. The researchers were not able to determine the underlying cause that permitted a treated or untreated patient with the chemical to reach hyper oxygenated states. The beauty and beast of science is that with every answered question paves the way to countless more unanswered questions. I left the lecture room a bit more confused than when I came in. But again, Dr. Harken’s objective of these lectures is to get you thinking and surely enough, he got me thinking.
The highlight surgery of my day goes to an incision and drainage of a right knee of a middle aged Filipino male. The patient’s knee had a large opening about a foot long that extend from his lower thigh, across his knee, and down to the middle of his lower leg. The doctors had the gash filled with a black absorbent sponge that was sutured in place. I have never seen this done before and was taken back at the site of the sponges as it appeared, from afar, as implants or ingrown black fungus patches on the surface of his skin. When I realized it was sponges, I breath a breathe of relief for the patient because for a moment I thought I was in some horror movie! What appeared as a wound from a freak accident actually had no collision based origin at all. Actually, the patient’s wound was caused by an initial bone infection I believed that ballooned up forcing the surgeons to cut open and operate on the leg. What complicated this injury even further was that the patient had diabetes that decreased the circulation in his legs which probably caused the patient to develop his end stage renal disease. End state renal disease is a condition where you kidneys are no longer function and you would need to have a kidney transplant or get kidney dialysis for the rest of your life. This would make recover and healing a difficult challenge for the patient and the doctors. The point of the surgery was to remove the sponges, drain the wound of blood and tissue debris, and then suture sponges back in. Thus they called this an incision and drainage operation. A big objective of the surgery was to acquire blood and tissue sample from various regions of the gash to test for infection. Even if all goes well, because of the patient condition, there is a great of amputation later down the road.
The surgeon for this operation was Dr. Billings who is the oldest and wises surgeon you will meet at highland hospital. Despite his age, Dr. Billings is very affable at heart, loves to travel, and will share his stories to those that have the pleasure of his company. The surgery initiated with the removal of the sutures that held the black sponge in place. Once the sutures were removed and the sponges were taken out, blood began to spill out. The blood was slowly mopped up after several towels, yet blood continued to drip out. There was so much blood lost that the patient needed a unit of blood. Once most of the blood has been wiped up, you can see the bones of the patient’s femur and the knee joint. The tissue that usually surrounds the knee was completely peeled of the bone through the entirety of the gash. Just from the sight of the opening itself instilled doubt in my mind of the patient’s ability to walk normally again in the future. It was pretty disturbing for me to watch Dr. Billings wipe down the bone and then suction off blood in between the bone and the flesh, flapping the flesh around. I remember cringing my eyes from the sight and sounds created by the undertaking. To my surprise, Dr. Billings was complimenting on how clean the wound was, once he removed all the thick coagulated blood wedged between the tissue and bone. Once I got desensitized to the sounds and sights of the surgery, I began to really see the beauty of it all.
Just when I thought things were wrapping up, Dr. Billings took out an instrument that looked like what I can best associate as an ACME ray gun from the cartoons I watched growing up. It had a round funnel like opening at the tip that appeared soft and functioned by both sprayed and suctioned fluids. The instrument was turned on and Dr. Billings was quick at work irrigating the gash and then sucking fluids right back up. After twenty minutes of cleaning the opening, the wound was considered clean enough for the samples of tissue and blood to be taken. Swabs were used to accomplish this feat, swabbing to extract tissue in between the bone and the tissue of the knee. Once everything was done, Dr. Billings began to suture the tissue up a little bit. He did not suture the entire opening closed but more to hold the tissues of the knee against the bone. The opening was still very much open and exposed to the air. More of the black sponge was cut into strips to stuff the opening. Some light suturing was done to keep the tissue and the sponge flush together. A giant clear tape cover was used to saran wrap, if you will, the top of the entire opening. A small hole was cut into the tape, a tube was inserted, and a compressed bulb was placed at the other end. The bulb at the other end function to create negative pressure and suck out any pooled blood and acting as an indicator of how much internal bleeding was occurring. I was astonished at the bulb because I have never seen it used in this manner before. In the end, the leg was wrapped up tightly and the swabs were sent out to pathology. I am crossing my fingers that pathology comes back clean so the patient can keep is leg.
This observational day was the longest time I spent at the OR, cranking in at monstrous 16 hours. Good practice for residency I thought. I had a very rewarding experience in the OR today. In my wake, I had the pleasure of observing a radial bone repair of the hand, a sentinel lymph node biopsy, a laparoscopic colonoscopy, a part of a total thyroidectomy, an inguinal hernia repair, and an emergency throat tumor removal. A shout out to Dr. Billings, Dr. McDonald, Dr. Boudreault, Dr. Lim, and the podiatric and medical students that is extremely helpful and approachable. I meet a lot of new and familiar faces today. Just another reason to be excited to be a part of OREX. Until next time, Jimmy out.
June 2012 (Part 1)
By Chris Villanueva, OREXer ’11-12
On my observation day, I was in general surgery with Dr. Chong and it was something else. During the meeting, Dr. Harken talked about how oxygen delivery is caused by cardiac output, which is the length and intensity of exercise. This factor helps increase our quality and quantity of life.
After this wonderful lecture, I went into the OR with Charlie, a UCSF medical student and Dr. Chong, who surprisingly was my doctor in Kaiser Hayward. He was going to take out my appendix, but that was ruled out. The first surgery that we saw was an umbilical hernia, where Dr. Chong had his whole finger in his belly. After watching this short surgery, the next patient came in with a right Colectomy. That patient had pre-cancer and they wanted to remove the risk of it growing into a tumor by taking that part of the colon out. I saw as they prepped the patient and most importantly go over the comprehensive surgical checklist. There was the “sign in,” which had a list of checkpoints before the patient transferred to the OR bed. The “time out,” which was another checklist before the patient is cut. Finally, the “sign out,” which was a list of checkpoints before the patient leaves the OR. For this surgery, they used a camera and microscopic instruments to cut and shear the colon without actually cutting her open.
The doctor cut part of the colon out until they finally removed part of the colon with the appendix through her belly button. Honestly, it was worth the six hour observation because it was huge, I thought it was going to be a small portion but it was huge and I got to see the appendix! After they took out the colon with the appendix, Dr. Chong finally came in and performed a reanastomosis. Charlie explained that a reanastomosis is when they connect two tubes together to help heal the colon and resume with proper bowel movement. He also explained that if there is too little colon, then they cannot perform a reanastomosis and as a result, a permanent colostomy bag is required. We would have a non- reanastomosis if there were too much cancer on the colon and we would not be able to connect it to another tube. This was one of my best observation surgeries.
May 2012 (Part 2)
By Tarik Afnoukh, OREXer ’11-12
I was late to the morning teaching; arrived around 8A.M to Highland and went directly to the OR. I saw Dr. Harken talking to Dr. Lim second year general surgery resident; so I joined the team for the rest of the day.
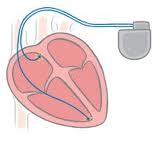
First patient was in her sixties complaining of chest pain. The patient had a Pacemaker 10 years ago because of third degree heart block and was stable until lately where the battery of the machine is no longer working which needed to be changed soon as possible. Let’s talk a bit about what is heart block? As the name says “Block” it means that the electrical drive pathway of the heart from Atriums to Ventricles is blocked somewhere (see picture 1). Usually the cause of this block is a fibrotic tissue came from either aging, side effects of medications, or diseases. We classify the block on three degrees. First degree there is slow electric conduction from atriums to ventricles, in the second degree there is an asynchronous between the atriums and the ventricles sometimes ventricles contract after atriums sometimes not, and the third degree is when the ventricles contract independently from atriums. To regain the heart beat synchronization, we need to coordinate between atriums and ventricles by a Pace Maker (means it will speed the electric activity from atriums to ventricles). It has two wires one connected to the inside of ventricle and the second to the inside of atrium, from that the machine will know instantly when the heart is contracting and which cavity is delaying (see picture 2). The surgery was easy and fast, after injecting of anesthetic drugs Dr. Lim made an incision on the old surgical scare and took out the old pace maker after disconnecting it from the wires that had been introduced to the right heart cavities and fixed a new machine in the same place.
The second patient was 62-years-old, with a history of Coronary Artery Diseases -had three stents on 2010- complaining of chronic and intermittent chest pain. A second degree heart block was diagnosed with a severe bradycardia 35 beats/min (it was a second degree type 2 or Mobitz II block). I talked to the patient in pre-op for awhile with her niece, a bit stressed but she was smiling at the end when the circulator came. After skin sterilization of the chest and neck, Dr. Lim made a small incision below the left clavicle guided by Dr. Harken. She stuck the left axillary vein and introduced a wire toward the right ventricle. X-ray with scope was used to make sure that we are in the vein toward the right heart not in the artery toward the left heart. First, Dr. Lim pushed a ventricular pace maker lead guided by the wire and the X-ray toward the right ventricle. A very funny technique; first we need to push the lead -we saw in the screen that the lead was driven by the blood flow to the pulmonary artery- from that we need the retrain the lead few cm until it became straight (not curved) then push it again “but fast this time” in the way that it will be driven by the blood flow from the atrium to the bottom of the ventricle; the lead has a hook like shape which can stick easily into the trabiculated (not smooth) ventricle wall. Second, is the atrium lead guided by the atrium wire and the X-ray, this lead should be fixed perpendicular to the ventricle lead. Dr. Harken explained for as with looking to the scope screen how the two leads move with the heart beat, first the atrium lead then the ventricle lead, if one of them move abnormally or lately; a signal will be transmitted to the Pacemaker which can synchronize it. After making sure that all leads were placed and fixed in the correct place, Dr. Lim connected the leads to the Pacemaker and fixed it in subcutaneous bellow the left clavicle. A technician from the Pacemaker’s company was there with a special machine to program the Pacemaker in the safe way for the case (depending on the heart rate and the energy consumed by the heart in each beat).
Third patient was a 64-year-old diagnosed recently with Tonsillar cancer, in the need of chemotherapy. A port-vein catheter is necessary to deliver medicine safely. I also talked to him in the pre-op station. He was not stressed but he was a bit upset about the anesthesiologist who didn’t find a good vein for IV. The patient’s mother and sister were there, we laugh a lot when I asked the sister is the patient related to you? She said yes “I am his brother” and then the mother said so “I am the Daddy.” After skin sterilization of neck and chest, Dr. Lim put a central line from the right jugular vein guided by ultrasounds and introduced a catheter through toward the right atrium, ideally into the superior vena-cava. She made an incision 2cm below the right clavicle where she fixed the chemo-chamber reservoir beneath the skin. It has a silicon septum where the nurse can stick needles easily and inject the chemo-drugs. To connect this chamber to the jugular vein catheter, the resident made a subcutaneous way, then passed and connected the catheter into it.
Fourth patient was a 70-years-old with End Stage Kidneys Failure who is in dialysis almost a year. He is a Mexican man, moved seven months ago to the USA to live with his son. I talked to him, he doesn’t speak English but the patient’s neighbor was translating to me and to the staff. He likes the US and he wants to stay here to the end of his life. He receives dialysis three times a week through a central line in the right subclavicular vein, which is at high risk of infection and sepsis. The surgery today is the arterio-venous fistula, where Dr. Lim and Dr. Harken made a fistula (a communication) between the Ulnar artery and the Ulnar superficial vein using surgical magnifying glasses. The Principal of the technique is that arteries are small, strong vessels with high resistance, and thick walls (for that we feel the pulses) but veins are large, weak vessels with thin and muscle-less wall (low resistance no pulse, for that veins can dilate easily and widely without rupture). So because arteries are strong vessels, when we communicate an artery with a vein; the high artery pressure will be transferred to the vein, but because the vein is low resistant, the wall will dilate –after surgery it becomes bigger and easier to stick a needle in to- Try to palpate a vascular fistula when you have a chance (like in the ED, usually patient is in room 12) you will feel a thrill indicating a high blood flow transferring. After making an incision in the lateral 1/3 lower left forearm, a superficial vein was readily under the skin but the Ulnar artery took some time to find, guided by its pulsation. Because of the patient’s age, Dr. Harken had pointed out for us a fibrotic tissue surrounding the patient’s blood vessels; we need to make sure that when we suture these vessels to keep the fibrotic tissue outside the lumen of the fistula (otherwise it can be a risk of fistula thrombosis).
The last patient was a 54-year-old patient hospitalized in the ICU; she had a third degree heart block in need of a pacemaker. The ICU staff brought the patient to the OR. The surgery had been in quick and safe conditions. Here the end of the Full day iVascular Surgery. 
1/Picture from ekginterpretation.com 2/Picture from icardiomg.com
May 2012 (Part 1)
By Tiffany Polar, OREXer ’11-12
Today I looked at the white board with great anticipation and excitement for seeing amazing surgeries. I scanned the surgeries for the day and the C4-C5 decompression soon caught my eye. I scrubbed in and prepared for the surgery. I wasn’t too certain exactly what C4-C5 decompression is or how the surgery will be performed but I was thrilled to learn. A cervical spine surgery seemed very risky. And cervical decompression sounded like they would be reducing the C4-C5 disc. I was immediately curious if they would be sawing the bone off to reduce some type of nerve pressure. I sat and watched the surgery team prepare the patient for surgery.
I was able to discuss the patient’s history with one of the nurses before the surgery began. I learned the patient had been having very devastating pain with the nerves in his hands and legs for several months now. The patient was in his middle 50’s and had numbness, tingling, and severe pain due to his C4-C5 disc degeneration. The nurse walked me to his X-ray to view the bone that had been putting pressure on the patient’s spine. Looking at the x-ray it became very noticeable how the bone was pushing against the spine. There was also another problem the patient’s C4-C5 disc had degenerated over some time, which was another cause of his pain. I could see the two bones almost sitting on top of each other with very little space in between, in comparison to the other bones which all had apparent space in between each one. The nurse informed me that aging caused this and there was no exact cause of the degeneration or the growth of the bone that had been pushing against the spine. She ensured that the surgeon would be able to cure both problems.
I learned the goal for the surgery was to first reduce the bone that had been putting pressure against the spine. This was done by a sort of sawing off of the bone back to a safe size relieving and reducing the pressure against the spine. It will no longer sit against the spine. Next the surgeon will insert a device to open the space between the bones that had degenerated and had fallen on top of each other. The device will be inserted and slowly opened to allow the necessary space between the bones. The surgery took about 4-5 hours and went smoothly. I was happy to know the patient would be relieved from the horrible pain he was receiving.
The next surgery I witnessed was a left breast tumor re-incision. It was a 37-year-old woman patient who had surgery several months prior to remove the cancerous cells. The doctors found suspicious cells and wanted to go back into the breast and remove more cells to ensure the cancer would not return. The patient was already prepped for surgery when I arrived into the Operation Room and the first incision into the breast was soon to happen. Two senior residents were performing the surgery under the direction of a surgeon. The residents seemed very skilled and it was clear they had performed this surgery before. This was interesting to view because the cells were removed via laser and suspicious lymph nodes were cut out. The surgery went smoothly and hopefully the cancer will not return.
